



 Español
Español  French
French  German
German  Hungarian
Hungarian  Italian
Italian  Português (BR)
Português (BR)  Português (PT)
Português (PT) Parodontale Risiko-Beurteilung
Die parodontale Risikobeurteilung bestimmt das parodontale Risiko des Patienten für ein weiteres Fortschreiten der Erkrankung und den anschliessenden Zahnverlust. Nach Lang und Tonetti (2003) bilden die folgenden sechs Parameter die Grundlage der parodontalen Risikobeurteilung.
Das Bluten auf Sondierung (BOP) wird durch leichtes Sondieren des Taschengrundes mit einer standardisierten Parodontalsonde bestimmt.
More …An vier Stellen pro Zahn wird vorsichtig sondiert. Die Anzahl der Taschen von 5 mm oder tiefer wird notiert.
More …Für die Zwecke der vorliegenden Risikoanalyse umfasst ein vollständiges Gebiss 28 Zähne (Weisheitszähne sind ausgeschlossen).
More …Der Prozentsatz des Knochenverlusts wird anhand von Röntgenaufnahmen der Seitenzähne geschätzt. Die Stelle mit dem grössten Verlust liefert den Wert für den Knochenverlust.
More …Die am besten belegten Hinweise auf eine Veränderung der Krankheitsanfälligkeit und/oder des Fortschreitens der Parodontitis stammen aus Studien an Populationen mit Diabetes mellitus Typ I und Typ II.
More …Der Konsum von Tabak, vor allem in Form von Rauchen, beeinflusst die Anfälligkeit und das Behandlungsergebnis von Patienten mit chronischer Parodontitis.
More …Online-Tool zur parodontalen Risikobeurteilung
Bluten auf Sondierung (BOP)
Das Bluten auf Sondierung (BOP) wird durch leichtes Sondieren des Taschengrundes mit einer standardisierten Parodontalsonde bestimmt.
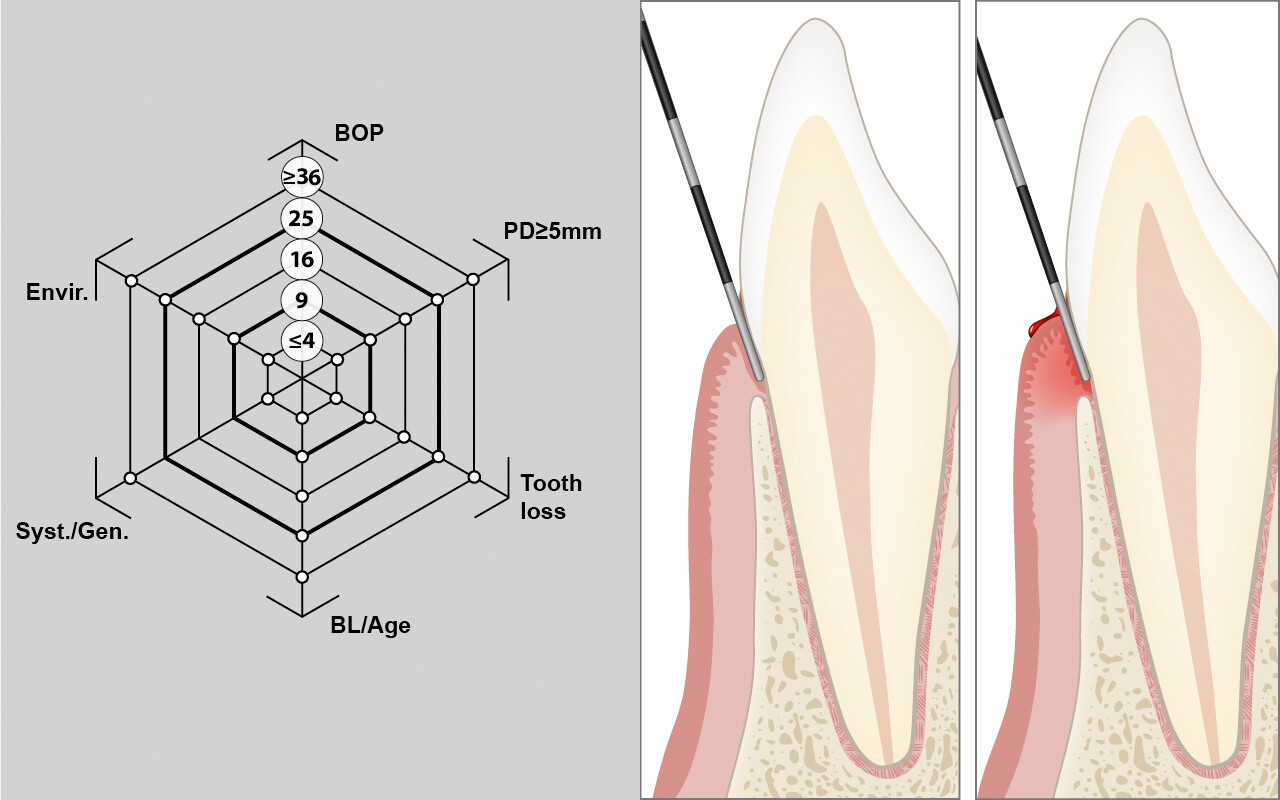
Das Ergebnis ist dichotom positiv oder negativ. Der ausgeübte Druck sollte 0,25 N (25 g) nicht übersteigen.
Das BOP wird an vier Stellen pro Zahn gemessen (mesio-bukkal, mid-bukkal, disto-bukkal und mid-oral). Dies geschieht am besten quadrantenweise, wobei zuerst die bukkalen und dann die oralen Messungen vorgenommen werden.
Der Bleeding-on-Probing-Score ergibt sich aus der Anzahl der positiven Stellen geteilt durch die Gesamtzahl der Stellen multipliziert mit 100.
Anzahl der parodontalen Taschen mit Sondierungstiefen ≥5mm
An vier Stellen pro Zahn wird vorsichtig sondiert (mesio-bukkal, mid-bukkal, disto-bukkal und mid-lingual). Die Anzahl der Taschen von 5 mm oder tiefer wird notiert.

Bei der Beurteilung des Risikos für ein Fortschreiten der Erkrankung wird die Anzahl der Resttaschen mit einer Sondierungstiefe von ≥5 mm als zweiter Risikoindikator für ein Wiederauftreten der Erkrankung im funktionellen Diagramm der Risikobeurteilung bewertet. Die Skala verläuft linear mit den Werten 2, 4, 6, 8, 10 und ≥12% als kritische Werte auf dem Vektor.
Personen mit bis zu 4 Resttaschen können als Patienten mit relativ geringem Risiko eingestuft werden, während Patienten mit mehr als 8 Resttaschen als Personen mit hohem Risiko für ein Wiederauftreten der Krankheit gelten.
Anzahl der verlorenen Zähne
Für die Zwecke der vorliegenden Risikoanalyse umfasst ein vollständiges Gebiss 28 Zähne (Weisheitszähne sind ausgeschlossen). Weisheitszähne, die mesial an die Stelle der zweiten Molaren gewandert sind, werden als zweite Molaren gezählt.

Die Anzahl der im Gebiss verloren gegangenen Zähne ohne die dritten Molaren (28 Zähne) wird gezählt, unabhängig von ihrem Ersatz. Die Skala verläuft ebenfalls linear mit 2, 4, 6, 8, 10 und ≥12 als kritische Werte auf dem Vektor.
Personen mit bis zu 4 verlorenen Zähnen können als Patienten in einer Kategorie mit geringem Risiko eingestuft werden, während Patienten mit mehr als 8 verlorenen Zähnen als Patienten in einer Hochrisikokategorie gelten können.
Prozentualer Knochenverlust im Verhältnis zum Alter des Patienten
Der Prozentsatz des Knochenverlusts wird anhand von Röntgenaufnahmen der Seitenzähne geschätzt. Die Stelle mit dem grössten Verlust liefert den Wert für den Knochenverlust.
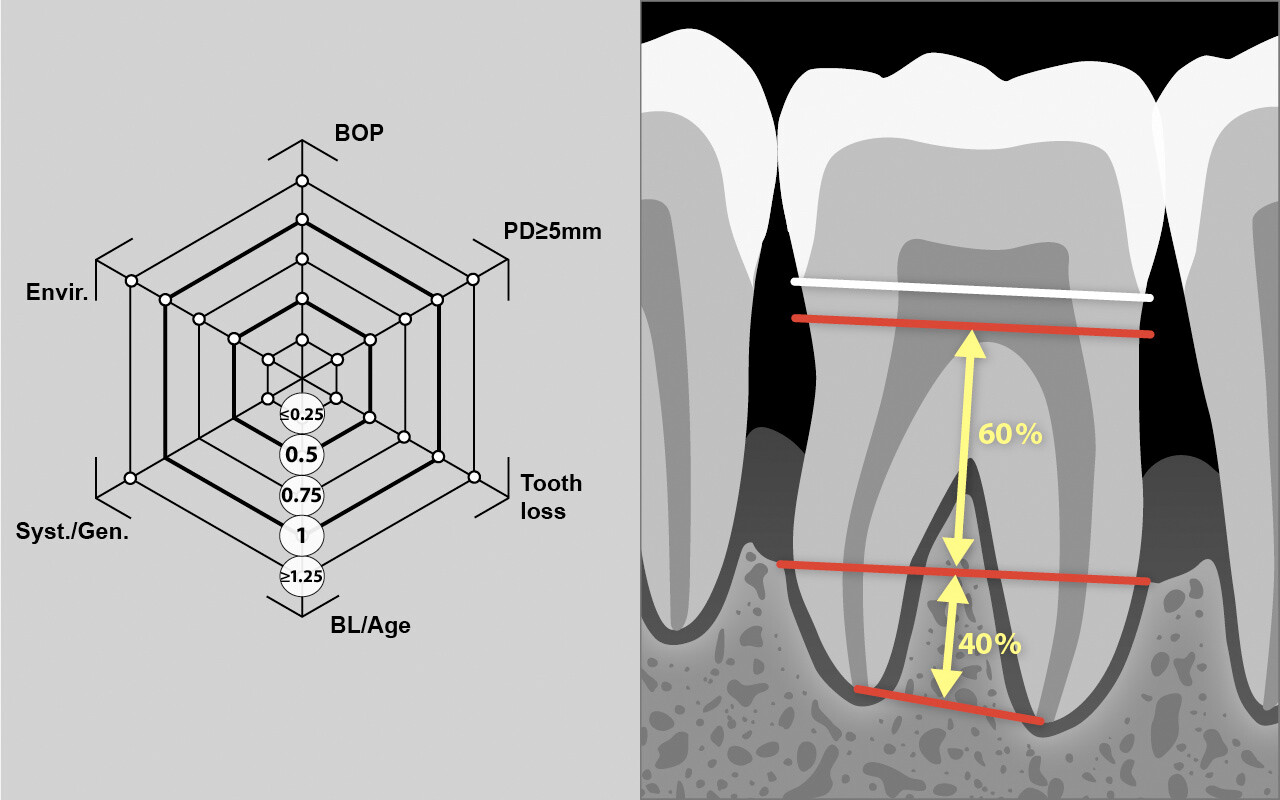
Das Ausgangsknochenniveau wird 1 mm apikal des CEJ angenommen. Der Knochenverlust wird grob in 10%-Schritten geschätzt. Falls keine periapikalen Röntgenaufnahmen vorhanden sind, können Bissflügelaufnahmen verwendet werden. Bei dieser Schätzung wird der Knochenverlust mit 10 % pro mm veranschlagt.
Bei der Beurteilung des Risikos für ein Fortschreiten der Erkrankung wird das Ausmass des Alveolarknochenverlusts im Verhältnis zum Alter des Patienten als vierter Risikoindikator gewertet.
Systemische Faktoren
Die am besten belegten Hinweise auf eine Veränderung der Krankheitsanfälligkeit und/oder des Fortschreitens der Parodontitis stammen aus Studien an Populationen mit Diabetes mellitus Typ I und Typ II (insulinabhängig und nicht insulinabhängig).

Es ist zu beachten, dass die Auswirkungen von Diabetes auf parodontale Erkrankungen bei Patienten mit unbehandelter parodontaler Erkrankung dokumentiert wurden, während bis heute keine eindeutigen Belege für behandelte Patienten vorliegen. Es ist jedoch davon auszugehen, dass der Einfluss der systemischen Bedingungen auch das Wiederauftreten der Krankheit beeinflussen kann.
Bei der Beurteilung des Risikos für ein Fortschreiten der Erkrankung werden systemische Faktoren, falls bekannt, nur als fünfter Risikoindikator berücksichtigt. In diesem Fall wird der Hochrisikobereich für diesen Vektor markiert. Falls nicht bekannt oder nicht vorhanden, werden systemische Faktoren für die Gesamtbewertung des Risikos nicht berücksichtigt.
Umweltfaktoren
Der Konsum von Tabak, vor allem in Form von Rauchen und nicht in Form von Schnupfen oder Kauen, beeinflusst die Anfälligkeit und das Behandlungsergebnis von Patienten mit chronischer Parodontitis.
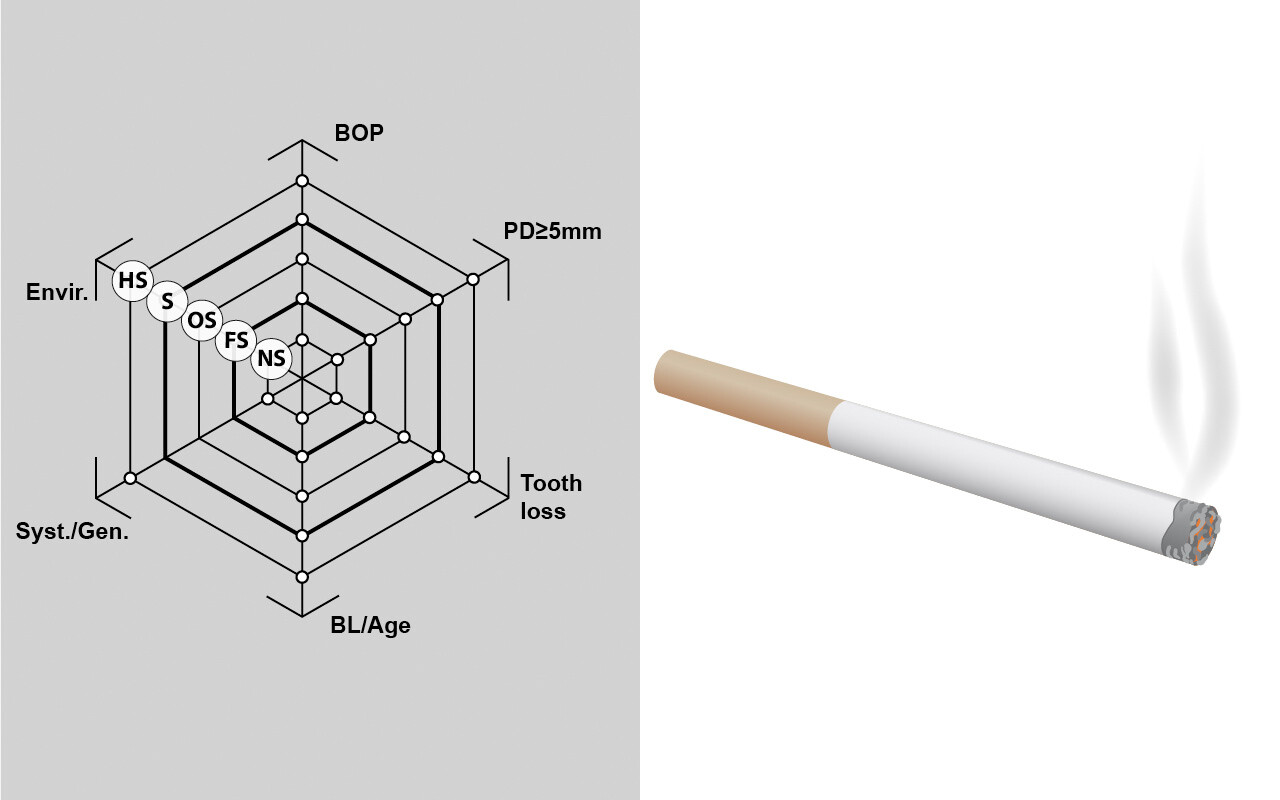
Bei der Beurteilung des Risikos eines Fortschreitens der Erkrankung müssen Umweltfaktoren wie das Rauchen als sechster Risikofaktor für das Fortschreiten parodontaler Erkrankungen berücksichtigt werden.
Trotz der wenigen verfügbaren Belege für den Zusammenhang zwischen Zigarettenrauchen und schlechteren Ergebnissen während der unterstützenden Parodontaltherapie (UPT) erscheint es angemessen, starke Raucher (≥20 Zigaretten/Tag) während der Erhaltungsphase in eine Gruppe mit höherem Risiko einzustufen.
Während Nichtraucher (NS) und Ex-Raucher (FS: mehr als 5 Jahre seit dem Aufhören) ein relativ geringes Risiko für ein Wiederauftreten der Parodontitis haben, besteht für starke Raucher (HS: definiert als Rauchen von mehr als einer Packung pro Tag) definitiv ein hohes Risiko.
Gelegenheitsraucher (OS: <10 Zigaretten pro Tag) und mässige Raucher (MS: 10-19 Zigaretten pro Tag) können als Patienten mit mässigem Risiko für ein Fortschreiten der Krankheit angesehen werden.
Referenz
LANG N P, TONETTI M S: Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent 1: 7-16 (2003).
Artikel herunterladenZusätzliche Informationen
Sie können unsere Inhalte für Ihre eigenen Produktionen unter Berücksichtigung der Creative Commons Lizenz verwenden:
Namensnennung - Nicht-kommerziell - Weitergabe unter gleichen Bedingungen 4.0
https://creativecommons.org/licenses/by-nc-sa/4.0/deed.en

Wie Sie unsere Inhalte zitieren:
www.perio-tools.com / CC BY-NC-SA 4.0